delta dental appeal form
The Appeal Request Form must be received by Delta Dental of Kansas within 180 calendar days from the. Ad Download or Email Enterprise Claim Form More Fillable Forms Register and Subscribe Now.
2
Because of the reason for denial listed on the last EOB issued _____ and because our patient talked to a representative for_____ and was told the claim should not have been denied.
. Delta Dental of California. The Appeal Request Form must be received by Delta Dental of Kansas within 180 calendar days from the date of the original adverse benefit determination or the corresponding remittance advice. Request for External Review Appeal Form 1B pdf 1 page Use this form for an external appeal review.
Delta Dental of New Jersey. Preventive care coverage varies by plan and by demographic considerations such as age. Locum Tenens Provider Form.
Delta Dental PPO participation packet request. Box 15132 Little Rock AR 72231 Attention Director of Customer Service Request for Review or faxed to Delta Dental at 973 285-4095 with a cover form addressed to Request for Re-Review within thirty 30 days following the Participating Dentists receipt of. Disputes not submitted on this form or lacking necessary information to resolve.
DeltaCare USA participation packet request. Delta Dental of Ohio is a part of Delta Dental Plans Association. Please refer to the vision appeals packet for information on submitting DeltaVision Administered by EyeMed appeals.
This form should only be used to submit an appeal. Appeal Request Form and Instructions Providers or members who wish to file a formal appeal related to an adverse benefit determination must complete the Delta Dental of Kansas Appeal Request Form. Pre-authorizations or referrals are required for certain benefit plans and certain dental care providers.
Delta Dental of New Jersey PO. We cover more Americans than any other dental benefits provider - and strive to make dental coverage more accessible and affordable to a wide variety of employers groups and individuals. How To Appeal A Claim Claim Appeal Information.
Preventive services are included in this tool. Use this secure form to file a grievance or appeal a dental benefits decision. Refer to your benefit plan to determine whether these requirements apply to you.
Fraud Waste and Abuse Attestation. Theres no hassle in working through claims saving you time and frustration. You will receive a written decision on your request for review within 30 days unless more information.
Re-Evaluation Committee 111 Shuman Blvd. Box 15132 Little Rock AR 72231. Exchange orthodontic medical necessity criteria.
After receiving this Appeal Request Delta Dental of Kansas will either send you a written decision regarding your appeal or if necessary request additional information regarding your. CLAIMS APPEALS SENT TO THE PO BOX WILL BE DELAYED. Appeals should be mailed to.
If you wish to file a dispute with Delta Dental please complete the form below include all supporting documentation and clearly identify why you are disputing Delta Dentals action or inaction. You will receive written confirmation of your grievance within 5 days. Request a copy of a check.
Appeals should be mailed to. Sale of Practice Notification Form. Delta Dental is Americas largest and most trusted dental benefits carrier.
Request for Internal Review Appeal Form 1A pdf 1 page Use this form for an internal appeal review. Disputes must be written and must clearly describe the basis of the dispute. CLAIMS APPEALS SHOULD BE SENT TO THE STREET ADDRESS BELOW NOT THE PO BOX.
With Delta Dental we keep you smiling. The law requires the following be placed on all plan grievance forms. Through our national network of Delta Dental companies we offer dental coverage in.
Continuous Orthodontic Coverage Form for DeltaCare USA. Dentist Directory Update Form. Register a Super User for your office today.
THE PO BOX IS FOR CLAIMS ONLY. Fraud Waste and Abuse Training Log. Combating Medicare Parts C and D Fraud Waste and Abuse Training Web Based Training Course 2021.
Delta Dental of Washington is a part of Delta Dental Plans Association. Authorization to Release Health Information Form Use this form to allow access to health information for adult dependents or a spouse. Delta Dental Premier Network Forms - Professional Application Credentialing form Delta Dental Premier Dentists Agreement Ownership Control Form and W-9.
Appeal Form - Information on how to appeal your claim. Use this form to file out-of-network dental claims. Through our national network of Delta Dental companies we offer dental coverage in all 50 states Puerto Rico and other US.
Removable Prosthodontics Assessment Form. Any request for re- review shall be in writing shall either be mailed to Delta Dental of New Jersey at PO. Dear Dental Appeals Consultant Per the request of our patient _____ we are reopening the appeal process for the attached claim with additional documentation.

Claim And Admin Forms Delta Dental

Delta Dental
2
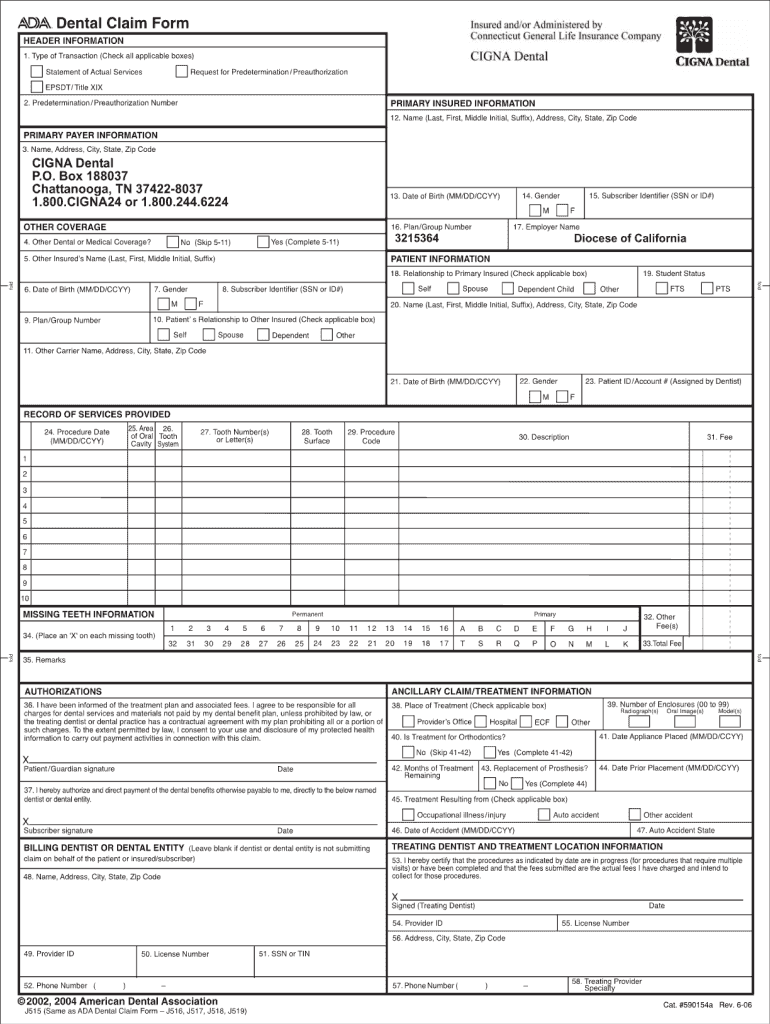
Cigna Dental Claims Address Fill Online Printable Fillable Blank Pdffiller

News Release Delta Dental Of Wisconsin
2

Pin On Cricut Templates
2
2
Dc 37 Dental Fill Online Printable Fillable Blank Pdffiller
2
2
2

Dc 37 Dental Fill Online Printable Fillable Blank Pdffiller
2
2

Sample Letters Of Appeal To Dental Insurance Lovetoknow

Pin By Dentaltown On Patient Education Dentistry Dental Health Dental Fun

Fillable Online Disabled Dependent Application Delta Dental Massachusetts Form Fax Email Print Pdffiller